At the age of 81, Mrs. Koesniyah was diagnosed with aggressive late-stage cancer that had spread to her lungs.
Biopsy results from a lump on her left neck showed non-Hodgkin’s lymphoma (NHL) type.
CT scan results showed septated lumps filling her right and left neck, especially the left side. Thorax X-ray results also showed nodules in her right lung. She was pushed in a wheelchair due to weak right motor function; there had been no examination regarding possible spread to the brain.
Due to age factor, Mrs. Koesniyah did not undergo chemotherapy; the only alternative at that time was using ECCT. Her condition gradually improved, the lumps softened until they were no longer palpable. She is healthy and relatively active at her age of 84 in June 2026.

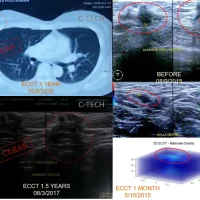
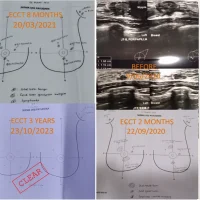
Figure 1: From right to left: Photo of Mrs. Koesniyah’s lump in the mandibular area extending to her neck before using the device, biopsy results showing non-Hodgkin’s lymphoma mass; and photos of the neck area 2 weeks, 2 months, and 1 year after using the ECCT device, showing the mass gradually softening and shrinking, without inflammation and with increasingly normal surrounding skin; Far right: Photo of Mrs. Koesniyah after 2.5 years (16/10/2025) using the device, showing a healthy and relatively active condition.
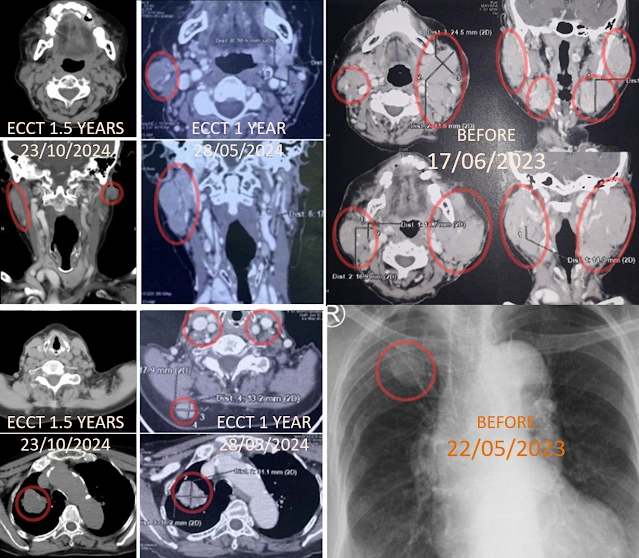
Figure 2: From right to left: CT scan results of the neck area showing lesions on the right and left lymph nodes in the cervical region before using the ECCT device (17/6/2023), X-Ray results showing lung lesions possibly caused by spread (22/5/2023), and CT scan results after 1 year and 1.5 years showing shrinking lesions in both the neck and lungs.
***
Three years ago, at the age of 81, Mrs. Koesniyah was diagnosed with aggressive late-stage cancer that had spread to her lungs. Inflamed lumps appeared on her right and left neck. She spoke little, unlike her usual self who tended to be talkative and loud.
Biopsy results from a lump on her left neck showed non-Hodgkin’s lymphoma (NHL) type. The biopsy wound had not dried and often still bled.
CT scan results showed septated lumps filling her right and left neck, especially the left side. Thorax X-ray results also showed nodules in her right lung. She was pushed in a wheelchair due to weak right motor function; there had been no examination regarding possible spread to the brain.
She felt embarrassed meeting her friends because of her swollen neck. Of course, such embarrassment was a luxury, as she should have been more concerned about her cancer which could be fatal. Especially given her advanced age, treatment options became very limited, compounded by Mrs. Koesniyah also having underlying conditions (comorbidities), a history of gallstones, liver cirrhosis due to hepatitis A, and pneumonia.
The prognosis in Mrs. Koesniyah’s case was classified as severe. Advanced age, stage IV lymphoma cancer (spread to the lungs), plus complications of lung infection (pneumonia) and co-existing conditions such as cirrhosis and gallstones, can significantly reduce tolerance to curative treatment and life expectancy.
The spread of cancer to the lungs indicates Late-Stage (Stage IV) Non-Hodgkin’s Lymphoma (NHL). This can worsen pneumonia, cause shortness of breath, and requires immediate management to control cancer cell growth and treat the lung infection. The tolerance of elderly bodies to aggressive therapies like standard chemotherapy tends to be lower and carries a risk of complications or toxicity. Liver dysfunction in cirrhosis makes drug metabolism (including chemotherapy drugs or infection drugs) more difficult and high-risk. Infections or inflammation in the lungs occurring simultaneously with cancer heavily burden the respiratory system and body’s immunity.
A multidisciplinary medical team (usually consisting of oncologists and internal medicine specialists) must balance the aggressiveness of cancer therapy with the patient’s quality of life (supportive/palliative care). Supportive care is crucial, such as administering antibiotics for pneumonia, transfusions if needed, pain management for gallstones, and liver protectant medications. For NHL, generally doctors might consider low-dose chemotherapy, targeted therapy, or corticosteroid therapy. The choice of therapy is adjusted based on the patient’s overall functional status (performance status).
Her doctors did not recommend chemotherapy due to her age and underlying conditions. Her family also did not want Mrs. Koesniyah to undergo chemotherapy. The only alternative at that time was ECCT. In general, high-grade cancers respond well to ECCT, with cells undergoing rapid death. If elimination proceeds smoothly, the cancer mass will slough off within days or weeks, marked by extreme elimination reactions such as dark/black, very pungent stools, and very pungent urine and other excretions; lumps gradually soften and shrink within days or weeks. The type of NHL experienced by Mrs. Koesniyah is a high-grade (aggressive) lymphoma, which responds quickly to ECCT; the relatively soft character of its dead cells (low calcium content, low cholesterol components) allows the dead cells to break down and be absorbed by the body’s immune system and excreted well through body excretions; tumor masses can soften and shrink within days or weeks.
The character of dead NHL cells differs from types with lower aggressiveness, such as classical Hodgkin’s lymphoma, which has relatively high cholesterol content, making it more difficult for the body’s immune system to absorb, prone to precipitation, and causing inflammation. From general observations, persistent inflammation is one of the crucial factors that can influence cancer progression, leading to fluctuating cancer conditions, making it difficult to achieve remission or progression-free status. For low-aggressiveness types, ECCT therapy generally still needs to be assisted by standard chemotherapy to suppress inflammation. Administering chemo after 2-3 months of ECCT use for classical lymphoma types typically quickly suppresses inflammation; significant mass reduction can occur with just the first 1-2 rounds of chemo.
The aggressive character experienced by Mrs. Koesniyah offers an advantage with ECCT therapy: cancer cells can die quickly, while her body’s burden to absorb and process dead cells is relatively light, and even at over 80 years old, she can still handle it. She was provided with an ECCT device in the form of a blanket and helmet covering her entire body up to her head, due to the extent of the spread and considering the possibility of wider dissemination.
Initially, she could only use the device for 15 minutes each morning and evening for 2 weeks. She complained of a burning sensation, especially in the lump area on her neck, abdominal bloating due to excessive gas, coughing, severe aches in her left leg, and dizziness when using the device. The effect of “cancer cells bursting instantly” when using the device can cause dizziness and pain, and the detox effect of accumulated dead cells in the body can be disturbing, causing coughing, bloating, or numbness in the hands or feet, before finally being expelled in the form of gas, urine, phlegm, and feces.
However, generally, her progress was quite fast, in line with good elimination reactions. The lump on her neck began to loosen and shrink within 2 weeks, the biopsy wound dried, and the inflammation decreased. Smooth elimination reactions are very important in the ECCT therapy process to achieve complete resolution. The accumulation of dead cells that are not expelled, in addition to causing various complaints, can lead to chronic inflammation which, if persistent, will trigger tumor cell development again. For cases where elimination reactions do not occur well, medical procedures such as chemotherapy, radiation, or surgery are still needed.
Fortunately, Mrs. Koesniyah experienced smooth elimination reactions, the lump gradually shrinking, and inflammation also disappearing. However, she did experience the emergence of a new lump on her right neck, which was initially almost clear. This was likely influenced by her fluctuating immune system, given her advanced age. The lumps on her neck only completely disappeared after using the device for approximately 2 years.
In May 2026, Mrs. Koesniyah passed 3 years since she was first diagnosed with stage 4 lymphoma cancer. Her condition is relatively normal and healthy. She is still active on social media, reading and sending WhatsApp messages, watching YouTube videos, attending regular religious study groups, gathering with friends and family, and engaging in physical activities such as walking, washing dishes, and tidying up the house.
At 84 years old, her memory is still excellent, her retention strong, and she can still debate political and economic issues both domestically and internationally. She continues to use the ECCT device not only to prevent cancer recurrence but also to maintain smooth blood circulation, prevent blockages in blood vessels in organs, heart, and brain, and preserve good memory.
May Mrs. Koesniyah remain healthy (WS).