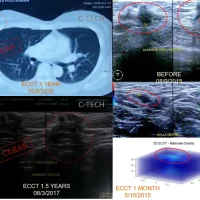
Mr. Roni’s neck cancer rapidly enlarged after diagnosis and continued to grow despite undergoing 6 cycles of chemotherapy, causing coughing, difficulty swallowing, and nightly chills. He was first diagnosed with cancer in early 2021. Biopsy results indicated a type of neuroendocrine cancer/diffuse non-Hodgkin’s lymphoma (poorly differentiated). Initially, he did not want to continue chemotherapy, but on the advice of an ECCT consultant to continue chemotherapy due to the excessively large mass, he resumed his chemo after starting to use the device. The cancer mass shrank rapidly with just one chemo cycle after using the device for 2 months first. After the second cycle of chemotherapy was completed and the mass had shrunk, he then continued using only the device to fully eliminate the remaining mass until clear and has now surpassed 5 years.

***
Mr. Roni and his wife initially refused further medical intervention with chemotherapy because, after diagnosis, the mass rapidly grew and continued to enlarge despite undergoing the first 6 cycles of chemotherapy. The large mass on his right neck caused coughing, difficulty swallowing, and nightly chills. He only wanted to use ECCT and did not want to continue the chemotherapy process as advised by his doctor.
CT scan results showed a mass almost 10 cm in size, compressing the common carotid artery and jugular vein, large blood vessels in the right neck already infiltrated by the mass. Biopsy results indicated a type of neuroendocrine cancer/diffuse non-Hodgkin’s lymphoma, which had already infiltrated striated muscle tissue (skeletal muscle), the primary muscle that functions to move the head and neck, including muscles that control overall neck movement, as well as deeper muscles related to swallowing and speaking. The CT scan also showed thickening in the right and left nasopharyngeal areas. The mass in the neck was suspected to be a result of metastasis from the nasopharynx, thus falling into the late-stage category. Surgical intervention was not recommended due to high risk and potential for wider spread, caused by its position already infiltrating the neck muscles and the possibility of metastasis from other sites.
This cancer is an aggressive type originating from neuroendocrine cells scattered throughout the body (lungs, digestive system, etc.), growing rapidly, and potentially spreading, characterized by abnormal cells that are difficult to distinguish from normal cells and require special tests for diagnosis. Symptoms vary depending on the location, and can include digestive problems, weight loss, skin flushing, fatigue, or respiratory problems, and are often difficult to diagnose early because they resemble other conditions. The prognosis for poorly differentiated/diffuse neuroendocrine cancer (NEC) is generally poor due to its aggressive nature, faster spread, and greater difficulty to treat.
For non-Hodgkin’s lymphoma (Diffuse Large B-Cell Lymphoma/DLBCL), this is the most common type of Non-Hodgkin Lymphoma (NHL), a cancer that attacks the lymphatic system (immune system) and grows rapidly in lymph nodes, spleen, bone marrow, or other organs, characterized by symptoms such as fever, night sweats, weight loss (B symptoms), and painless lumps in the neck, armpit, or groin. The prognosis for this type of lymphoma is generally better than for NEC.
Killing cancer cells with ECCT is relatively not a major problem; cells undergo rapid death, especially for high-grade ones. However, too many dead cells in the body can cause an excessive burden due to a cytokine storm, which refers to proteins produced by immune cells to deal with dead cells.
The C-Care Research consultant explained that for an excessively large mass, the body might not be able to absorb dead cells and naturally excrete them through metabolism. Therefore, medical intervention is necessary to prevent chronic inflammation, involving a combination of chemotherapy to suppress the immune response.
Mr. Roni and his wife accepted the advice to use ECCT while continuing medical procedures, specifically chemotherapy, as initially examined by his oncologist. He began using the device for 2 months before continuing the second cycle of chemotherapy for 6 sessions over 4 months, while still using the device.
The lump significantly shrank immediately after the first treatment of the second chemo cycle. He completed his chemotherapy, finishing 6 sessions in one cycle, while continuously using the device. PET scan results after 6 months showed the lump in his neck had shrunk from 10 cm to 2-3 cm. Other parts of his body were relatively clear, with no detected spread.
Mr. Roni continued to use ECCT alone to completely eliminate the remaining lump in his neck until it was clear, after 2 years of use since he first started using the device.
His condition is relatively normal. His body weight has returned to what it was before he fell ill. We hope Mr. Roni (WS) stays healthy.