Previously, his father passed away from colon cancer, and later he, his older sibling, and his child were diagnosed with the same cancer. He was the first to recover from the cancer, having lived 10 years cancer-free after using ECCT without chemotherapy, and then encouraged both his sibling and child to use ECCT without chemotherapy.

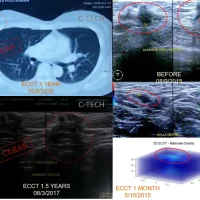
Image: Left: A photo of Mr. Ismanto accompanying his son during a consultation with Dr. Warsito (April 3, 2014); Right: A CT scan image and a photo of the surgical scars from Mr. Ismanto’s 2014 operation.
In early 2014, at the age of 42, Mr. Ismanto was diagnosed with colon cancer. The fear he had been living with became a reality. His father had previously passed away from the same type of cancer, after undergoing surgery followed by chemotherapy. Now, he himself faced the same disease that had taken his father’s life.
Initially, he complained of being unable to defecate for several days. His stomach grew large due to waste accumulating in his intestines. A CT scan revealed a blockage in the transverse colon. What appeared to be waste was filling his intestines, swelling and occupying much of his abdominal cavity.
A biopsy conducted at a hospital in Ponorogo showed malignancy: adenocarcinoma with poor differentiation—the most aggressive type of colon cancer.
Unable to defecate, he had no choice but to undergo a 35 cm colon resection. Fortunately, his intestines could be reconnected, so he didn’t need a colostomy bag installed on the outside of his abdomen, which would have to be carried around for life.
For life? Yes, for life, if the intestines couldn’t be reconnected, which is common for tumors located near the rectum or anus. In Mr. Ismanto’s case, the tumor was located far enough from the anus, so reconnection was possible.
However, with the type of cells in Mr. Ismanto’s case, that might not provide much help. Adenocarcinoma with poor differentiation is an extremely aggressive type that spreads diffusely (making it visually indistinct), easily recurs, and spreads widely. Mr. Ismanto did not want to face the same fate as his father.
But medical science had no effective solution for colon cancer, especially for an aggressive type like Mr. Ismanto’s. The only option was surgery followed by chemotherapy.
The prognosis for this type of cancer, even with surgery and chemotherapy, remains poor. The chances of surviving up to 5 years are only 20-40%, while 60-80% do not survive past 5 years. That was the case for his father, who passed away shortly after surgery and chemotherapy. Living with a “colostomy bag for life” was still considered fortunate because “for life” could mean a short period.
The pathology analysis from Mr. Ismanto’s surgery revealed an even more worrying result: high-grade malignant fibrohistiocytoma, a type of sarcoma located in the colon, more malignant than adenocarcinoma. It was unlikely that chemotherapy would help much.
A month after his surgery, Mr. Ismanto began experiencing hardening around the surgical area of his abdomen. It seemed the cancer was quickly growing back. He didn’t want to meet the same end as his father and sought alternative treatments.
In early 2014, ECCT was a topic of much discussion. Mr. Ismanto resolved to use ECCT, without chemotherapy. He became one of the first to use ECCT for colon cancer, hoping that ECCT would replace chemotherapy and eliminate any remaining cancer cells post-surgery.
Fortunately, the type of cancer Mr. Ismanto had was relatively quick to respond to ECCT, including both the poorly differentiated adenocarcinoma and the sarcoma. Both are highly aggressive types, but the more aggressive the cancer, the quicker the cells respond to ECCT. This leads to faster breakdown of cells (dissolving into dead cells in liquid form) and excretion as mucus along with feces.
After obtaining the ECCT device at CCare Alam Sutera, Mr. Ismanto returned to his home in Ponorogo. There was no further news from him for 10 years.
It wasn’t until early 2024 that he returned to CCare. His condition was well and healthy, very normal. He had never undergone the chemotherapy that his doctor recommended. He used the ECCT device for 2-3 years initially and never returned for consultation or device checks afterward. But 10 years later, he was still alive and well.
It seems that ECCT was quite helpful, especially for highly malignant cancers, requiring only a few months of use to clear remaining cancer cells post-surgery without the need for chemotherapy. This was similar to what Mrs. Suwarni, the first ECCT user, did—surgery followed by ECCT without chemotherapy.
This time, Mr. Ismanto returned to consult for two people: his older sister and his son. Both of them had the same type of cancer that he and his father had—colon cancer. Both had already undergone surgery. Mr. Ismanto wanted them both to be cancer-free like him, using ECCT after surgery without chemotherapy.
Mr. Ismanto’s sister and son had been using the device for 2 months, and their progress was promising; both were in healthy and normal condition.
Wishing good health for Mr. Ismanto and continued progress for his sister and son (WS).