Mr. David (44) was diagnosed with kidney cancer in early 2015. His entire left kidney had turned cancerous, with a tumor mass measuring over 12 cm. The cancer had also spread to his right kidney, where a lesion measuring 4 cm was detected, categorizing the cancer as stage 4. Mr. David underwent a nephrectomy to remove his entire left kidney. The right kidney, which also showed signs of cancer, was left untreated. His doctor recommended chemotherapy after the surgery to slow the growth of the mass in the right kidney and to prevent the recurrence or further spread of cancer in the left kidney area.
However, the chances of eliminating the mass in his right kidney with chemotherapy alone were slim. There was a possibility he would also need to undergo another surgery to remove his only remaining kidney and hope for a kidney transplant. Faced with this serious risk, Mr. David opted for an alternative path using ECCT (Electro-Capacitive Cancer Therapy) to avoid both chemotherapy and the removal of his last kidney.
In the early stages of ECCT use, Mr. David experienced some kidney function disturbances, but he later went through the therapy smoothly without any major complaints. Routine CT and MRI scans consistently showed no recurrence at the site of the removed kidney and no spread to other organs. The mass in the right kidney remained relatively stable in size and gradually transformed into tissue resembling normal kidney tissue. After five and ten years of ECCT therapy, Mr. David remained in excellent health and led a normal, active life.

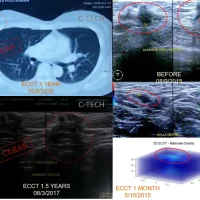
TOP: Initial CT scan showing a large mass in the left kidney (over 12 cm) before surgery and a lesion in the right kidney; MRI result after one year of ECCT post-nephrectomy showing no recurrence or spread, with the right kidney mass relatively unchanged; CT scan after five years of ECCT showing similar conditions. BOTTOM: Ultrasound image of the right kidney after ten years of ECCT, showing a mass of relatively stable size and texture resembling surrounding normal tissue, and a photo of Mr. David in a healthy, normal state.
As the first known case using ECCT for this condition, Mr. David approached the therapy cautiously but remained highly optimistic, even without prior case studies, considering that research and past cases had shown ECCT could destroy malignant cells without damaging healthy ones.
About 90% of kidney cancers are renal cell carcinoma (RCC), a type that begins in the small tubes inside the kidney. This type of cancer usually arises when waste blockages damage the walls of these narrow tubes over time. The body attempts to repair the damaged walls through healthy cell division. However, if the damage remains unresolved, continuous cell division may result in “protein expression errors,” turning the cells cancerous.
Renal cell carcinoma can typically be cured if detected early and treated appropriately. Standard treatment includes surgical removal of the tumor—usually the entire kidney—followed by ablation, radiation, and/or chemotherapy to eliminate any remaining cancer cells that might have entered the bloodstream or lymphatic system, and to prevent recurrence or further spread. Complete remission—meaning no recurrence or spread—is generally only possible for early-stage cases (stages 1–2). For stage 3, this is possible only if the entire tumor is successfully removed with no spread. In stage 4 cases like Mr. David’s, medical recovery is considered nearly impossible due to the cancer having spread to other organs, blood vessels, and lymph nodes. According to the American Cancer Society (ACS), the five-year survival rate for metastatic kidney cancer is only 15–17%.
Alternative cancer treatments such as ECCT are not limited by the extent of metastasis. Actively dividing cancer cells can still be destroyed by the electric field generated by ECCT devices—even if they’ve spread to other organs, blood vessels, or lymphatic tissue. Unlike chemotherapy or targeted drugs, ECCT’s electric fields are not limited by areas without large blood vessels—such as the peritoneum, lymphatic tissue, or fat (omentum)—which are common sites for cancer recurrence after kidney cancer surgery. The electric field can penetrate tissue matrices and target active cancer cells.
However, ECCT’s electric field therapy generally does not affect healthy cells, including the tumor’s supportive (stromal) cells. In kidney tumors, malignant cells often only comprise a small portion of the outer layers, while the majority of the mass is made up of recruited healthy support cells, forming the tumor’s “shell” or structure. Malignant cells respond rapidly to ECCT, dying off and being excreted through urine—which may appear foamy and have a strong odor, as Mr. David experienced early in the therapy. Still, because the majority of the tumor mass consists of slower-dividing supportive tissue, it remains relatively unaffected by the electric field, resulting in little to no change in tumor size—even though the cancerous cells die off quickly (within 3–6 months).
In Mr. David’s case, CT scans over the first five years showed the tumor mass size remained stable, with no signs of distant spread or recurrence at the surgery site. Periodic ultrasounds from year five to year ten revealed the mass tissue slowly transforming from solid to a fluid-mixed texture resembling normal kidney tissue. This regeneration into normal cells—similar to what is seen in surface cancers like breast cancer—may also occur in kidney cancer, as evidenced in Mr. David’s case.
Mr. David experienced kidney function issues at the beginning of the therapy, but his function returned to normal as the treatment progressed. Animal studies have shown that ECCT not only destroys malignant cells but also helps improve kidney and liver function. After five and ten years with ECCT, Mr. David remains in very good health and continues to lead a normal, active life. May he remain healthy and active (WS).