Rangdra was only 11 years old when he was diagnosed with malignant cancer in the spinal cord (medulla spinalis) in his neck area in 2012. A biopsy revealed medulloblastoma. He underwent radiation treatment, but two years later, the cancer recurred. He underwent radiation again, along with chemotherapy, but ended up paralyzed and unable to walk, relying on a wheelchair. After exhausting all medical options, the doctors recommended using the ECCT device. Rangdra became the first case of medulloblastoma (spinal cord cancer) to be treated with ECCT therapy.

Rangdra was only 11 years old when he was diagnosed with malignant cancer in the spinal cord (medulla spinalis) in his neck area in 2012. A biopsy revealed medulloblastoma. He underwent radiation treatment, but two years later, the cancer recurred. He underwent radiation again, along with chemotherapy, but ended up paralyzed and unable to walk, relying on a wheelchair. After exhausting all medical options, the doctors recommended using the ECCT device. Rangdra became the first case of medulloblastoma (spinal cord cancer) to be treated with ECCT therapy.
In mid-2012, Rangdra complained of neck stiffness, unable to turn it freely. Initially, he thought it was just a bad sleeping position or muscle soreness. However, the pain worsened over time. His parents took him to see a neurologist at a private hospital in Jakarta. An MRI scan revealed a mass in the spinal cord area in his neck.
Rangdra then underwent a series of radiation treatments. After the radiation, his condition improved, and his symptoms subsided. He was able to return to his normal daily activities.
However, this only lasted for less than two years. At the beginning of 2014, his symptoms reappeared, this time more severe. He returned to the doctor who initially treated him. The MRI results showed that the tumor had grown back, larger than when it was first detected. He underwent 30 more radiation sessions, followed by 6 rounds of chemotherapy.
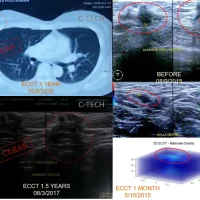
Unfortunately, his condition did not improve after the second round of radiation and chemotherapy. Instead, he became paralyzed, unable to stand or walk. He had to rely on a wheelchair, and his daily activities became increasingly limited. The latest MRI after radiation and chemotherapy showed that the tumor had grown to 10 cm X 2 cm X 2 cm, with his spinal cord diameter tripling in size compared to normal.
Since all available medical procedures had been exhausted and the tumor still gripped the central nervous system in Rangdra’s spinal cord, the doctors finally wrote a recommendation letter to C-Care Research for Rangdra to begin ECCT therapy.
Rangdra’s treatment continued with ECCT, closely monitored by his doctors. A few days after starting the therapy, he experienced extreme reactions. His bowel movements were black and foul-smelling, his sweat was sticky with a strong odor, and his urine was cloudy and had a pungent smell.
Along with these intense eliminations, Rangdra’s condition improved, and his symptoms lessened. A few weeks after starting the device, he began to move his legs, and within a few months, he learned to stand again. After a year, he could walk on his own and no longer needed the wheelchair. An MRI scan after two years showed the tumor had shrunk to under 1 cm in diameter from the original 2 cm, and the length had reduced from 10 cm to less than 7 cm. The tumor had mostly turned into cystic fluid, forming increasingly thin islands.
Medulloblastoma is an invasive tumor that grows rapidly. Unlike most brain tumors, it spreads through cerebrospinal fluid and often metastasizes to various locations along the surface of the brain and spinal cord. Metastasis to the cauda equina at the base of the spinal cord is referred to as “drop metastasis.”
The response to ECCT was fast, in line with the tumor’s aggressive growth. The elimination of dead cells also posed relatively few issues, as the dead cells flowed downward through the cerebrospinal canal to the base of the spinal cord and into the blood vessels along the spine, being expelled through the body’s excretions such as sweat, urine, and bowel movements. Overall, ECCT treatment for this case had relatively few challenges as long as Rangdra’s general condition remained stable.
Survival rates are cumulatively 60%, 52%, and 47% at 5 years, 10 years, and 20 years for all age groups and histological subtypes, with children faring better than adults.
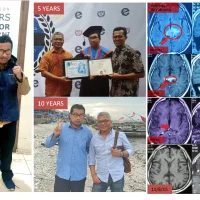
Once Rangdra regained his ability to walk, he became less frequent at C-Care as he became busy with school again, continuing his education that had been interrupted by treatment. He completed his elementary education successfully, then continued to junior high, senior high, and eventually college.
After a long absence from C-Care, Rangdra returned in mid-2024, marking 10 years of using the ECCT device. His condition was relatively normal, with only mild complaints of spondylosis in his spine. Otherwise, he was in good health. An MRI scan in 2017 had declared him cancer-free. He has since completed his studies in IT and now works as a Data Science expert.
Wishing continued health for Rangdra and that he remains a source of pride for his family.