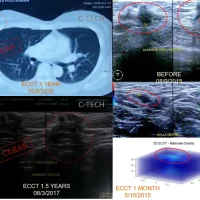
Diagnosed with advanced lung cancer at an advanced age (64 years), Mrs. Soewarti had limited treatment options. Her doctor prescribed oral chemotherapy and recommended therapy with ECCT. Three months after using the ECCT device, the tumor mass was no longer detectable. However, four years later, following the pandemic and after receiving several vaccinations, the tumor reappeared and increased in size. She resumed ECCT therapy with a new device tailored to the characteristics of the new tumor.

Diagnosed with advanced lung cancer at an advanced age (64 years), Mrs. Soewarti had limited treatment options. Her doctor prescribed oral chemotherapy and recommended therapy with ECCT. Three months after using the ECCT device, the tumor mass was no longer detectable. However, four years later, following the pandemic and after receiving several vaccinations, the tumor reappeared and increased in size. She resumed ECCT therapy with a new device tailored to the characteristics of the new tumor.
Soewarti (64) was diagnosed with lung cancer in mid-2019. Initially, she experienced persistent shortness of breath for two weeks, despite receiving medication from her doctor. She was then taken to the hospital, where an X-ray and CT scan revealed massive pleural effusion in her left lung, which made it difficult for her to breathe. The CT scan showed a 3 cm mass in the superior lobe of her left lung, with metastasis to the lymph nodes in the mediastinum (middle chest), possibly causing the massive pleural effusion.
A biopsy confirmed a malignant cancer, specifically adenocarcinoma, known for its poor prognosis. The average life expectancy for stage 4 lung cancer is less than a year, with a 5-year survival rate of only 5%. Treatment options for advanced lung cancer were very limited, and Mrs. Soewarti’s doctor only prescribed oral chemotherapy.
Due to the limited treatment options, Mrs. Soewarti’s doctor recommended using ECCT. Before starting ECCT therapy, fluid was drained from her lungs, as it not only caused severe shortness of breath but also interfered with the ECCT electric field therapy. The ECCT device’s electrical field flattens in the presence of fluid in the lungs, reducing or nullifying the electric force acting on the tumor. However, pleural fluid production generally persists even after drainage and only ceases after 3-4 months of ECCT device use.
The ECCT device Mrs. Soewarti used included a vest for targeting the lung mass and a helmet to prevent metastasis to the brain. ECCT is always applied with a coverage area that targets the primary tumor and potential secondary and tertiary metastasis areas. Mrs. Soewarti was advised to use the device for only 2×15 minutes per day for the first two weeks. This usage time was reduced compared to earlier ECCT devices, which were used for up to 16 hours daily.
After three months, the 2-3 cm tumor mass was no longer detectable on the new X-ray. Her shortness of breath and other symptoms disappeared in a relatively short time. She returned to normal activities, even stopping the oral chemotherapy prescribed by her doctor. However, during the COVID-19 pandemic from late 2020 onward, Mrs. Soewarti rarely attended follow-up appointments. She continued to use the ECCT device for preventive measures even though the tumor had shrunk and ceased growing.
She began to experience shortness of breath again after receiving several vaccinations during the pandemic. Her chest pain worsened on the left side. New X-rays and CT scans showed tumor growth in the original tumor site, which had remained unchanged for three years. In addition to the original site, several new lesions were detected in her left lung. The new tumor had a different character compared to the original mass from four years prior, consisting of multiple lobulated lesions adhered to the pleural wall and near the heart. The recurrence of the tumor could have been caused by a bronchial obstruction following vaccination, potentially due to fibrosis (scar tissue) that formed after the death of the initial tumor mass.
The vaccine’s effect is not directly responsible for the emergence of cancer, but the blood flow obstruction in the fibrotic area could lead to the accumulation of the vaccine, resulting in continuous inflammation and the emergence of malignancy.
Due to the different tissue type in the new tumor compared to the initial mass, Mrs. Soewarti received a new device in mid-2023 tailored to the new cell type. The latest device was effective in removing fluid from the lobulated tumor mass. Her vest was replaced with a blanket-like covering for more effective treatment coverage. She began ECCT therapy again with the upgraded device. After three months, the lesions started shrinking, and some of the newly formed lesions had already disappeared.
By mid-2024, exactly five years since her initial lung cancer diagnosis, Mrs. Soewarti’s condition was very healthy. She was active, and her recent CT scan showed further tumor shrinkage, with some masses remaining unchanged from the previous year.
Wishing you long-lasting health and happiness for Mrs. Soewarti.