A story of a woman who had to undergo surgery on both breasts due to cancer. After the first mastectomy followed by chemotherapy, the cancer returned in the other breast. She successfully overcame her cancer and surpassed 10 years after stopping chemotherapy and using ECCT.

Mrs. Sonti, a breast cancer survivor, has been using ECCT for 10 years.
Mrs. Sonti underwent her first mastectomy in 2013 to remove her right breast. The results of the surgery indicated malignancy. She then continued with chemotherapy until it was completed. The surgical scar dried and developed into a keloid.
Just a few months after surgery and chemotherapy, in early 2014, a lump reappeared—this time in her left breast. The ultrasound showed signs of malignancy, though it was unclear if it was a spread from the right side or a new occurrence. Besides the lump in her left breast, there was also a lump on her shoulder, about 2-3 cm in size, suspected to be benign, with characteristics resembling a lipoma.
Mrs. Sonti did not return to her initial doctor who had performed the surgery and chemotherapy. She decided not to undergo chemotherapy again and opted to use the ECCT device instead. She traveled a long distance from her home in Mandailing Natal, North Sumatra, to Tangerang to acquire the ECCT device.
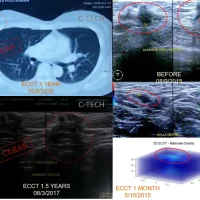
In January 2014, she began using an ECCT device in the form of a vest to cover her entire chest, along with a small device to cover the armpit area. At that time, ECCT was still in its early development stages, and its response was not yet classified by cancer type, nor was the device customized as it is today.
Mrs. Sonti did not experience typical elimination reactions common among ECCT users, such as strong-smelling sweat, dark and foul-smelling stools, and cloudy, pungent urine.
The electrical activity scan of her breast using ECVT also showed fluctuating numbers, sometimes increasing during menstruation. The lump in her breast also did not change much and even tended to grow. Nevertheless, Mrs. Sonti remained confident in the ECCT device and continued using it.
After 1.5 years without any change, but also no indication of spread to other organs based on X-ray and ultrasound results, Mrs. Sonti eventually decided to undergo surgery. The surgical results showed malignancy: Invasive Breast Carcinoma Grade 1.
After the surgery, she chose to continue using only the ECCT device, rejecting chemotherapy even though the surgeon recommended it after reviewing the pathology results. She felt confident using only the device without chemotherapy after seeing the case of Mrs. Suwarni, the first ECCT user, who underwent surgery and used the device without chemotherapy.
Her decision proved to be correct. Her surgical wound dried quickly after she resumed using the device, and there was no recurrence as had happened previously in her right breast.
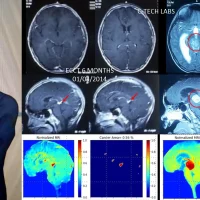
A year later, a comprehensive examination, including thorax X-ray, abdominal ultrasound, and bone scan, returned normal results. The surgical scars dried and formed keloids. Around the keloid area, dead black skin tissue appeared and dried like crusts on both the left breast and the right breast, which had previously undergone chemotherapy. The characteristics were similar to tissues exposed to radiation but only in certain areas around the keloid.
It is possible that there was a recurrence of the tumor mass around the surgical scars, both from the initial surgery on Mrs. Sonti’s right breast, which had undergone chemotherapy, and on the left breast, which did not. However, the cells that grew were later killed by the ECCT device. The cell death occurred more naturally in the malignant cells that re-emerged, unlike the remnants of radiation that leave dead tissue throughout the entire post-radiation area.
Mrs. Sonti later learned why her initial progress did not show reactions typical of other ECCT users. She discovered that her cancer cell type differed from Mrs. Suwarni’s case, being Invasive Ductal Carcinoma Grade 3. Research on electrical activity using ECVT indicates that the grade (malignancy level of cancer) is directly proportional to electrical activity—more aggressive cancer shows higher electrical activity. Consequently, the response to ECCT electric field therapy also varies; the more aggressive (higher electrical activity), the faster the response to ECCT. And vice versa.
This explains why Mrs. Sonti’s cancer type, Grade 1, with the lowest malignancy level on a scale of 3, showed a relatively slow response to ECCT electric field therapy. This type generally achieves remission faster when surgery is performed first, followed by using the ECCT device to clear any remaining cells or cells that may have entered the bloodstream and circulated throughout the body.
Mrs. Sonti’s approach proved to be right. She passed both the 5-year and 10-year remission marks without any recurrence, and her condition remained normal. She is very active and healthy.
Wishing continued health to Mrs. Sonti (WS).