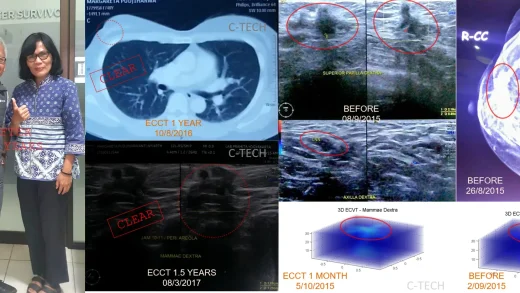
In 2012, Mrs. Herin was diagnosed with a meningioma-type brain tumor located right behind her eyes, in the area between her right and left eyes, known as the sella and suprasella regions. Surgery couldn’t remove all of the tumor. It recurred, spreading throughout the suprasella area, gripping her optic nerves, and attaching to the brain stem, causing her vision problems. Worse, her doctor informed her that she might not survive more than six months. A second surgery was not an option, and there were no other alternatives. She began using ECCT (Electro-Capacitive Cancer Therapy) at the end of 2012. The tumor stopped growing after using the ECCT device, but it wasn’t easy for Mrs. Herin to accept that her tumor could not be completely removed, her vision couldn’t fully return, and she had to come to terms with relying solely on her left eye for sight. After ten years, the tumor appears unchanged. Mrs. Herin continues using the ECCT device. Despite her vision problems, she remains healthy and active.

Rightmost image: MRI scan shows recurrent tumor mass post-surgery in the sella and suprasella regions extending to the brain stem; the tumor remains relatively stable and has tended to shrink after 5 and 10 years (Middle image); Leftmost image: Mrs. Herin appears healthy and active in a 2024 photo after nearly 12 years of using ECCT.
In 2011, Mrs. Herin underwent brain tumor surgery for a tumor located directly behind her right eye. Due to the tumor’s position affecting her right optic nerve, the surgery impacted her right eye’s vision, making it non-functional. She could only rely on her left eye for vision.
However, this didn’t last long. Less than a year after surgery, she began experiencing issues with her left eye. An MRI scan at the end of 2012 revealed a recurrent meningioma tumor mass occupying the area behind her right eye, extending into the skull bone behind her eye (sphenoid), expanding to the central brain area (intrasellar), pressing on hormone glands, and spreading to the right cerebral lobe.
The recurrent mass and its extensive spread to surrounding areas made a second surgery impossible. The spread to the cerebrum and pressure on hormone glands could also prove fatal, and her doctor mentioned that she might not survive beyond six months.
Initially, the benign tumor had become invasive, making its cells resistant to therapies like radiation and chemotherapy. After it was determined that a repeat surgery was not possible and there were no further medical options, Mrs. Herin decided to try ECCT in March 2013.
In general, benign or low-grade malignant tumors do not respond well to electric field therapy such as ECCT. This is because benign cells are less sensitive to electricity than high-grade malignant cells. Normal cells have the lowest electrical sensitivity compared to benign or malignant tumor cells.
Electrical sensitivity levels correlate with electrical activity during cell division. The higher the malignancy (high grade), the greater the activity level, making the cells more sensitive to external electric field disruptions, which can lead to cell death when stimulated to interrupt cell division, resulting in programmed cell death (apoptosis).
Normal or benign cells have lower electrical activity and a slower proliferation (cell division) rate. Therefore, the effect of cell death is also slower. For cases like Mrs. Herin’s meningioma tumor, the best achievable outcome is halting the tumor’s growth. For benign tumors, it is likely that the tumor mass won’t disappear with ECCT alone without surgery.
In addition to inhibiting tumor growth, ECCT also helps detach tumor masses from surrounding tissue, making them easier to remove surgically. Generally, using ECCT for 3-4 months is sufficient to loosen the mass that clings to surrounding tissue.
However, in Mrs. Herin’s case, performing surgery after recurrence and beginning device use would still be high-risk because the recurrent growth had already gripped vital tissues and organs around it. The story would be different if ECCT had been used before surgery; an initial surgery could likely have been cleaner, with a smaller chance of recurrence if the device were used continuously after the operation.
Mrs. Herin chose not to undergo a second surgery. She decided to use only the ECCT device, accepting the reality that the tumor mass could not be removed, and that her right eye was non-functional. She has had to come to terms with relying solely on her left eye, which already has some visual impairment.
Fortunately, indications of invasion into the cerebral lobe disappeared after one year of use, according to an MRI result in early 2014. The pressure on her hormone gland and brain stem from the front also decreased.
An MRI scan after 5 years of use showed that her tumor had stopped growing since she began using the ECCT device. After ten years, the tumor appears relatively unchanged, slightly shrinking.
Mrs. Herin continues using the ECCT device. Despite her vision problems, she remains healthy and active. Wishing Mrs. Herin continued good health (WS).