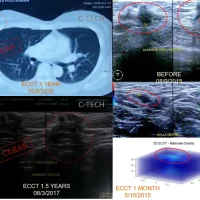
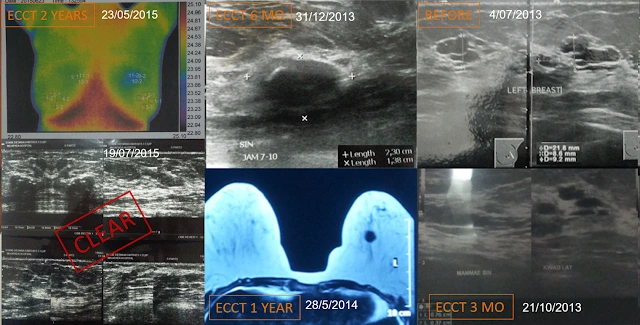
In 2013, Mrs. Syane developed lumps, both large and small, in her left breast, which tended to be malignant and benign. Because she did not want a biopsy or surgery, she only used ECCT while regularly performing check-ups with USG, MRI, and other radiological modalities, both standard and new. The lumps disappeared after using ECCT for 2 years, strengthening the suspicion that they were malignant because ECCT relatively does not react to benign masses and normal tissue. However, 3 years later, a lump appeared in her thyroid, 5 years later a lump also appeared in her kidney, and 8 years later, a lump also appeared in her right breast. What she did remained the same: Stay calm, continue using the device, perform routine monitoring. After 12 years, the results of routine monitoring concluded: the lumps suspected to be malignant disappeared with ECCT, while the benign ones remained relatively unchanged; and clearly, Mrs. Syane’s general condition has always been healthy and active.
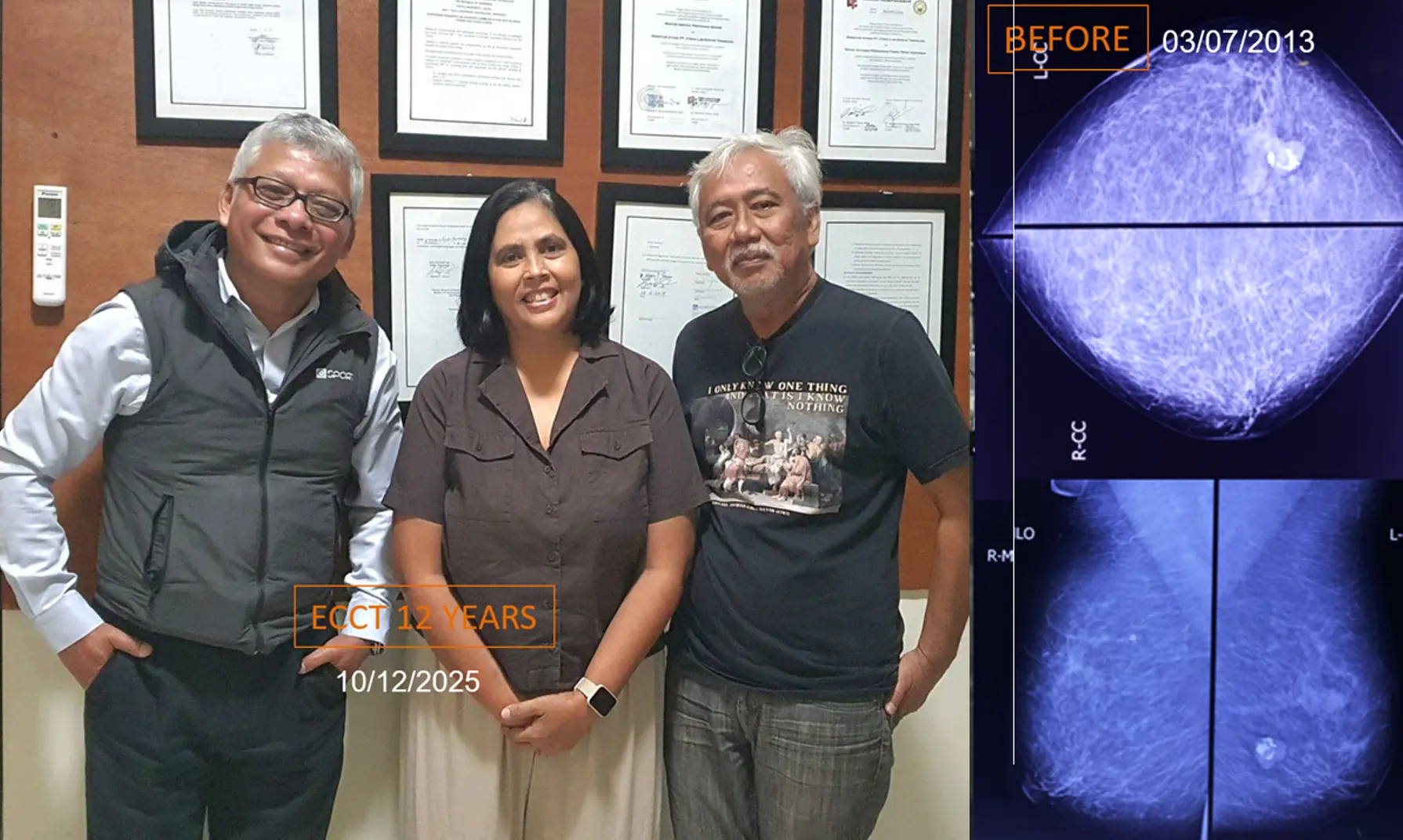
Image: Photo of Mrs. Syane in a healthy and active condition and mammography results from 12 years prior before using the ECCT device, showing a calcified lump tending to be malignant; BOTTOM from right to left: USG results of multiple complex mass and cystic before using ECCT, as well as USG and MRI scan results after 1 and 2 years of use, showing the mass shrinking until undetectable.
A lump was first detected in the left breast 12 years ago, then another appeared in the thyroid 3 years later, followed by one in the kidney 5 years after that, and another in the right breast 8 years later following a COVID vaccination. One thing Bu Siyane did not want to undergo was a biopsy or surgery.
So what did she do that allowed her condition to remain stable and healthy until now? How could a potentially malignant lump even disappear?
Using the ECCT device alone—without biopsy or surgery on breast lumps or other organ masses—may still allow the mass to disappear, depending on the cell type. In general, for high-grade malignancies (grade 3–4) with a pattern of cell death that disintegrates and can be absorbed by the immune system and excreted through urine, feces, and sweat (Group B/C1 according to ECCT response classification), lumps may resolve without surgery, and surrounding tissue can return to normal. This is based on a study by Prof. Shinichiro Akiyama et al., published in the World Academy of Anti-Aging and Regenerative Medicine (WAARM) Journal in 2024.
For other types, such as encapsulated lesions (Group A/E1) or dense/hard types with high cholesterol or calcium components (Group D/C2), ECCT alone is generally insufficient. These require combination with surgery or standard medical therapy for complete removal. Particularly for tumors characterized by positive estrogen receptor (ER), progesterone receptor (PR), and strongly positive HER2 on immunohistochemistry (IHC), targeted medications remain necessary to suppress the driving factors in addition to using the device.
Specifically, ECCT shows good response in Group B/C1 cell types characterized by ER-, PR-, and HER2-negative status (triple-negative). For other types, ECCT may still provide benefit if the lesion size is relatively small (less than 1–2 cm), depending on location. For larger masses, clearance of dead cells is often incomplete, especially for types other than B/C1. Inadequately cleared necrotic cells may leave dormant cells within the necrotic tissue, which can reactivate if triggering factors (strong ER, PR, HER2 positivity) remain high.
How can cell characteristics and therapeutic response be determined without biopsy and IHC testing?
Twelve years ago, IHC testing was not widely practiced, and ECCT-based response classification had not yet been established. What Bu Siyane did was routine non-invasive radiological monitoring using ultrasound, mammography, MRI, and even non-standard modalities such as thermography and ECVT (electric-field-based tomography). With consistent monitoring, any unfavorable progression could be detected early and anticipated.
Based on early ultrasound and mammography findings, the cell type in Bu Siyane’s case was categorized as Group E1—characterized by small encapsulated lesions that may spread to other organs. This type generally aligns with HER2-positive characteristics, which typically do not respond well to electric field therapy such as ECCT. For this type, ECCT ideally should be combined with anti-HER2 targeted therapy for optimal effectiveness.
However, because Bu Siyane did not undergo biopsy or IHC testing, the exact cellular characteristics were never definitively known. She chose to rely solely on ECCT for the potentially malignant lump in her left breast, as well as for subsequent lumps in the thyroid, kidney, and right breast. She focused on routine observation. As long as there was no progression toward deterioration, she felt aggressive intervention was unnecessary.
Her response was relatively slow, consistent with E1 characteristics. The lesion in her left breast remained relatively unchanged during the first year, and even showed slight enlargement within the first 3–6 months. She did not panic and continued calmly with the process. After two years, ultrasound results showed that the mass was no longer detectable. On physical examination, the lump was also no longer palpable.
Typically, lesions of this type are not considered highly responsive to ECCT. The favorable outcome in her case was likely because the lesions were relatively small (under 1–2 cm). Small lesions, even if multiple, can still be effectively managed by the immune system, allowing dead cells to be cleared properly. Additionally, psychological condition, hormonal balance, and cholesterol levels—which influence vascular plaque formation and clearance mechanisms—were likely well controlled, contributing to her successful outcome.
If hormonal activity is high and cholesterol levels lead to plaque formation in blood vessels, clearance of dead cells may be incomplete. Some cells may remain dormant rather than fully destroyed, potentially triggering recurrence. This may have occurred in Bu Siyane’s case after the COVID-19 vaccination, when a lump briefly reappeared, possibly due to inflammation and deposition in the scar tissue area of the previous mass. However, continued use of the device resulted in the lump disappearing again and reverting to scar tissue.
The thyroid and kidney lumps, which were likely benign, showed minimal change over 9 and 7 years of device use. ECCT tends to respond slowly to benign masses, but at least may help prevent progression.
From Bu Siyane’s case, an important lesson can be drawn: determining cell type early through biopsy and IHC testing remains valuable for accurate assessment of tumor characteristics and therapeutic response. With accurate cell typing, the worst-case scenarios, timing of progression, and best possible outcomes can be better predicted. Concerns about biopsy-related spread may be mitigated by using the device before and after the biopsy procedure.
Combination with standard medical therapy tailored to the specific cell type remains recommended and, in general, provides the best survival statistics based on another study conducted by Prof. Akiyama of McGill University, Canada, published in Frontiers in Medical Case Reports (2025).