Ovarian cancer is the deadliest gynecological cancer and the third most common cancer affecting women, with a low survival rate—60% of patients do not survive more than five years. For advanced stages like Mrs. Ida’s, where the cancer has spread to the bones, the survival rate is even lower. However, Mrs. Ida has successfully overcome this deadly cancer, living more than 11 years in a normal, cancer-free condition.

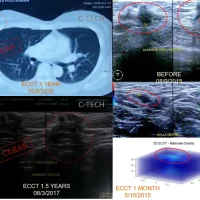
Ultrasound images of Mrs. Ida’s abdomen before and after using ECCT for 2 months, and MRI results after using the device for 3 months

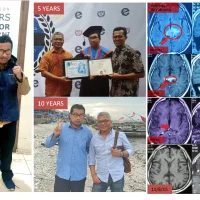
CT scan results after 5 years, and a photo after 10 years since being first diagnosed with ovarian cancer.
Mrs. Ida initially complained of an enlarged abdomen, appearing as if she were five months pregnant. An ultrasound revealed a complex mass filling the lower abdominal cavity. The doctor said it was difficult to operate on because it was adhered to the intestines and other vital organs throughout the pelvic cavity. The tumor marker for uterine cancer (CA 125) was 1107, indicating a high likelihood of malignancy. This occurred in late August 2012.
Even if surgery were performed, it was unlikely to remove all the cancer, necessitating follow-up chemotherapy. However, even with this treatment, regrowth was almost certain because the surgery wouldn’t completely eradicate the cancer.
Ovarian cancer is the deadliest gynecological cancer and the third most common cancer affecting women, with a five-year survival rate of only around 40%. This means that 60% of patients do not survive beyond five years. For advanced stages like Mrs. Ida’s, the survival rate is even lower.
The lethality of this cancer is due to its high recurrence rate and its tendency to spread to other organs. Once the cancer spreads to other organs, treatments like chemotherapy become ineffective.
Aware that surgery would be difficult, Mrs. Ida and her husband consulted with Dr. Warsito at his research center in Modernland, Tangerang. At that time, ECCT technology was widely covered in the media, which reported that ECCT could treat cancer without surgery or chemotherapy.
Dr. Warsito explained that her type of cancer was not like breast or brain cancer, which could be expelled without surgery; it was a mixed solid and cystic type encased in a membrane. “It cannot be expelled; surgery will still be necessary,” he explained in early September 2012.
“The doctor said it’s inoperable due to the adhesion to the intestines and other tissues,” said Mrs. Ida.
“We can create an ECCT device for you to use for 3-4 months, which will help loosen the adhesions so that surgery becomes possible. Afterward, you should proceed with surgery,” said Dr. Warsito.
“Don’t panic if your abdomen enlarges quickly and your tumor marker rises drastically,” he added.
“The abdomen will enlarge quickly over 1-2 months due to the solid malignant cells breaking down into fluid after using the device. However, because the dead cells are encased in a membrane, the body’s immune system will respond by producing immune fluid to attack them, causing the fluid to accumulate within the membrane, and the tumor will ‘balloon,’” explained Dr. Warsito.
“The tumor marker will also increase drastically because some of the dead malignant cells will pass through the membrane and enter the bloodstream, as detected by the marker test,” Dr. Warsito emphasized.
“Has this ever happened before?” Mrs. Ida asked hesitantly.
“No, you are the first case of this type,” said Dr. Warsito nonchalantly.
“But perhaps you have no other choice since the only medical option is surgery, and your case is currently inoperable due to adhesions,” he clarified.
“Although there has never been a similar ovarian case like yours, there has been a case of a cyst in the breast. The phenomenon should be similar since, from a physical standpoint, it is the same,” Dr. Warsito explained from his office on the second floor of his research center in Modernland, Tangerang.
“Alright then, I will try it,” Mrs. Ida finally agreed, with her husband, Mr. Husein, affirming her decision.
Mrs. Ida was provided with an ECCT device in the form of a pair of shorts, connected to a small AA battery-powered oscillator (electric wave generator). She was instructed to use it for 16-20 hours a day, almost non-stop.
The reaction she felt when using the device was pain in her lower abdomen, but it was bearable. A few hours after wearing the device, she experienced continuous gas expulsion at a very high intensity. Several days later, a mucous discharge appeared, similar to vaginal discharge. There was little reaction in terms of elimination through dark or black-colored bowel movements, sweat, or pungent urine.
After using the device for two months, her abdomen doubled in size but felt relatively softer than before, and the pain in her lower abdomen greatly subsided. Although this aligned with Dr. Warsito’s earlier explanation, Mrs. Ida still panicked, as she appeared to be in advanced pregnancy.
What panicked her even more was that her tumor marker test results had increased more than fourfold, from 1107 before using the device to 4792 after two months of usage. The ultrasound showed that many parts of the previously solid tumor had become fragmented and filled with fluid, indicating widespread necrosis.
“Keep using the device,” said Dr. Warsito.
Mrs. Ida continued using the device for another month and then underwent an MRI in preparation for surgery.
The MRI results showed a large mass measuring over 21x20x16 cm, with a relatively flat shape and a dominant fluid component compared to the initial mass, which was mostly solid with some fluid components. However, there were indications of spread to the spine, and she was declared stage 4.
“I think the results are quite good. Surgery may now be possible. You can consult your surgeon for the operation,” said Dr. Warsito.
“What about the spread to the bones?” Mrs. Ida asked worriedly.
“Immediately start using the device again after the surgery,” replied Dr. Warsito.
Mrs. Ida followed his advice and consulted her surgeon. After reviewing the MRI results and examining her abdomen, the surgeon scheduled the operation for early 2013, on January 2nd.
The surgery went smoothly; there was no adhesion, and all the masses could be completely removed. A total of five large and small sacs weighing around 5 kg were extracted. Because the surgery was clean, the doctor did not recommend chemotherapy and declared the cancer stage zero, reduced from the stage 4 diagnosis based on the MRI.

Image: Right: MRI results of the lower abdomen after 3 months of using the device before surgery, indicating spread to the spine; Left: Resulting ovarian mass cleanly removed after 3 months of device usage.
Mrs. Ida continued using the ECCT device to eliminate any remaining cells and address the possible spread to the bones.
After the surgery, everything returned to normal for Mrs. Ida. She resumed her work and usual activities. She was declared in remission less than 6 months after being diagnosed with ovarian cancer, following a combined therapy of using the ECCT device (3-4 months), undergoing surgery, and continuing device usage for preventive measures.
Mrs. Ida continued to use the device for 5 years as a precaution. A CT scan after 5 years in 2017 showed clear results, with no recurrence or spread.
In early 2024, Mrs. Ida reached the 11-year mark since being declared in remission and returned to Dr. Warsito with a similar complaint: “My abdomen is large.”
“Ma’am, I’m sorry, but this is a different issue, not related to cancer but rather fat—probably from eating too many fried foods,” Dr. Warsito responded.
“Okay, we can make another device to help break down abdominal fat, but it won’t have much ‘effect’ if you don’t reduce the fried food intake, especially at night,” continued Dr. Warsito.
Mrs. Ida continued her journey to reduce her abdomen size using electric fields, this time with a corset device worn around her abdomen during activities or even while sleeping.
May Mrs. Ida continue to stay healthy and active.
(WS).