Diagnosed with stage 2-3 breast cancer in 2013, Mrs. Margareta kept looking for alternative ways to avoid surgery until she found ECCT. She started using ECCT in 2015, and the lump disappeared within 1 year. However, 10 years later, after COVID and vaccination, the lump reappeared in the original mass site, which had turned into a keloid. She then only used the ECCT device again until it was clear again and only the keloid remained.
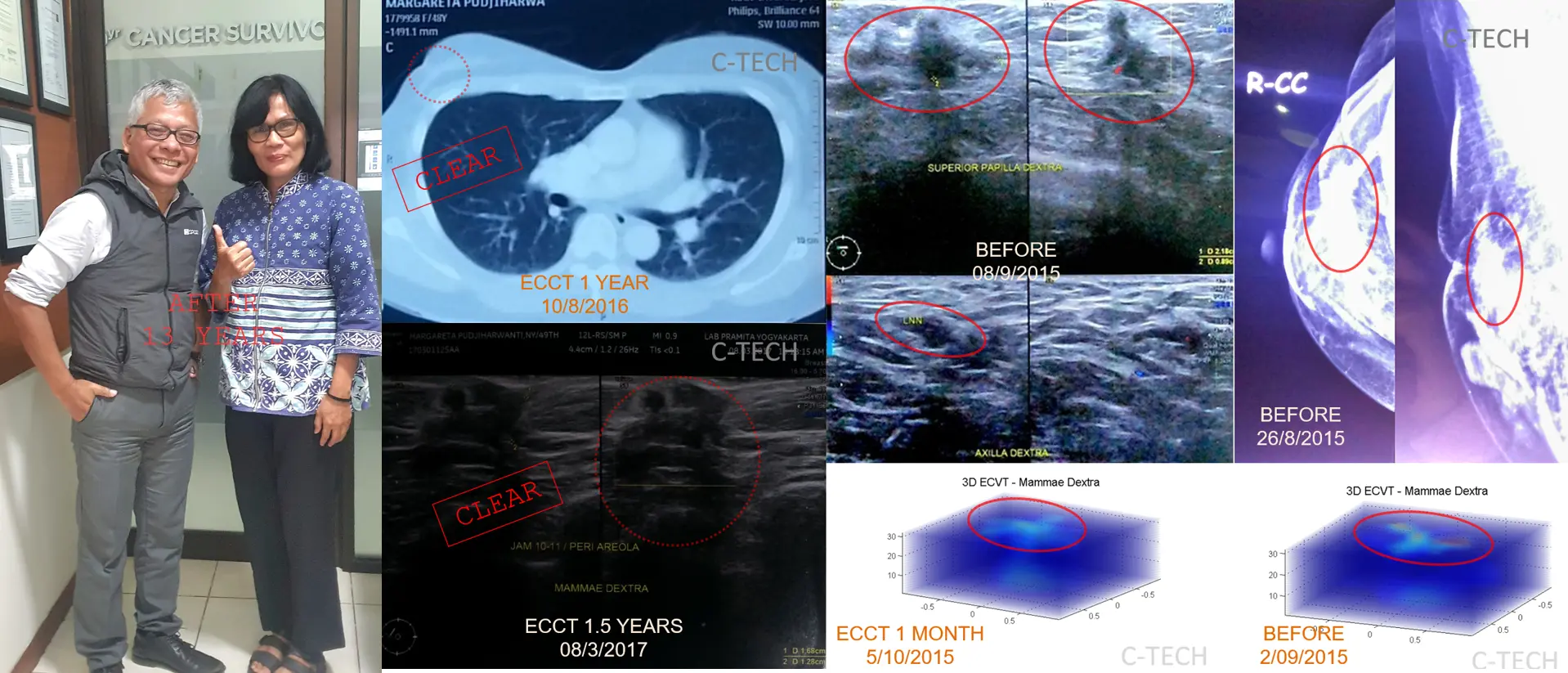
IMAGE:
Top right: Mammography and ultrasound results from 2015 after 2 years of alternative therapy before using the ECCT device, showing a persistent lump in the right breast with increasingly deep retraction at the site of the previous surgery; Bottom right: ECVT scan results of the right breast showing high electrical activity before ECCT use and a month after use, indicating a decrease in electrical activity; Middle: CT scan results after 1 year of ECCT use and ultrasound after 1.5 years, showing no detectable nodule like in the scan results before using the device; Left: Photo of Mrs. Margareta 13 years after her initial breast cancer diagnosis or 11 years after using ECCT.
***
Upon arriving in Penang, having flown all the way from Tambolaka, Sumba, NTT, Mrs. Margareta was told by her doctor: “There is nothing more to be done, Ma’am. The cancer is gone, only a keloid remains.”
Finally, Mrs. Margareta explained that she had been using ECCT. Her doctor continued: “Just keep using the device.”
Mrs. Margareta was diagnosed with breast cancer in 2013. Ultrasound and mammography results showed a lump in her right breast. Fine-needle aspiration biopsy (FNAB) results indicated malignancy. Her doctor suggested a mastectomy, with the possibility of subsequent chemotherapy and/or radiation.
Mrs. Margareta did not follow her doctor’s advice. She opted for alternative therapy for 2 years. She reported that her condition improved with the alternative therapy. However, the lump did not disappear. Ultrasound and mammography results after nearly 2 years of alternative therapy showed a persistent lump in her right breast, measuring 2-3 cm, with a small spreading lesion in the axilla measuring less than 1 cm. Retraction at the site of the previous surgery and the nipple increased. In terms of staging, it was still at stage 2-3, relatively similar to 2 years prior.
Generally, its progression over 2 years could be considered controlled. According to modeling studies, if left untreated, breast cancer with moderate malignancy naturally progresses from stage 2 to 3 within 18 months (1.5 years), and from stage 3 to 4 (metastasis) within 9 months.
She continued to search for alternative therapies to avoid surgery until she finally met ECCT. She flew from NTT to Tangerang to obtain the ECCT device in September 2015, bringing with her the latest mammography and ultrasound examination results as well as old biopsy results.
The response of breast cancer to ECCT depends on the cell type and degree of malignancy, based on Sahudi’s cell study results (2015). The higher the degree of cell malignancy (proliferation rate), the faster the cell death response with ECCT. A higher degree of cell malignancy correlates with a higher cell electrical activity index, based on electrical activity measurements with ECVT directly on patients in 2015. This is because during cell division (mitosis), cells experience a high increase in electrical voltage (potential) during mitosis, cells seem to “glow,” parts of the cell undergo electrical polarization, positive electrical charges at the chromosome position attach to kinetochore microtubule filaments in the mid-line area of the dividing cell, while negative charges are at both poles of division (centrosomes) in the peripheral area of the cell, chromosomes are pulled by
microtubule filaments from the center of the cell towards both poles of division through electrostatic attraction and repulsion. The electrostatic force occurring is very weak at the beginning of division but increases sharply towards the final phase of division, making it easily influenced by an external electric field if it is still in the early phase (before telophase). The effect of a weak external electric field can inhibit chromosome separation,
resulting in division failure leading to programmed cell death (apoptosis). Healthy cells relatively do not divide, so they are relatively unaffected by external electric fields. Cells with a low degree of malignancy have low electrical activity and a low cell division rate (proliferation), thus also a low level of influence.
Cells with a high degree of malignancy that fail to divide undergo complete cell death (apoptosis); dead cells can be well absorbed by immune cells and expelled from the body in the form of excretions such as urine, sweat, and feces, which sharply change in both color and odor. Cells with a low degree of malignancy, with the same electric field strength, experience more moderate damage, resulting in only partial cell damage and less complete cell death, with cells undergoing necrosis (forced damage), and generally, excretion reactions such as urine, sweat, and feces are not very noticeable.
Observing excretion reactions serves as an easy indicator to monitor the therapy response with the device. A good response can be detected within 1-2 weeks or even 3-4 days. If the excretion reaction is good, it can indicate that the cell character has a high degree of malignancy. Generally, good excretion will be followed by relatively rapid mass shrinkage within 3-4 months, and the device can be continued until complete. Conversely, if after 2-3 weeks the excretion reaction is still not very apparent, it can be indicated that the cell character corresponds to a low degree of malignancy; generally, the mass size does not change significantly even if therapy is continued, or the mass size can even enlarge due to necrosis (forced cell death) that is not properly expelled.
The excretion reactions experienced by Mrs. Margareta appeared in her urine, sweat, and feces, which were relatively more pungent but not overly extreme. The excretion character was consistent with a moderate degree of malignancy. Along with the excretion reactions, ultrasound results showed the lump size decreasing from 2 cm to 1 cm within 1 month, a relatively rapid shrinkage rate, consistent with a moderate to high degree of malignancy. ECVT scan results also showed a decrease in the electrical activity index compared to the previous month before using the device. CT scan results after one year of use showed no visible mass in her right breast; retraction in the area of the previous needle biopsy was still present but reduced, relatively smoother. Ultrasound results also showed only a residual shadow at the previous lump position, possibly due to dead cells that had transformed into remaining cholesterol deposits. Physically, mild keloid was visible in the needle biopsy area; otherwise, the breast condition seemed to return to normal.
Mrs. Margareta did not undergo a core biopsy (core biopsy) and immunohistochemical (IHC) testing to identify hormonal factors and HER2 receptor characteristics, so her cell type and trigger factors are not accurately known. The response characteristics of cancer cells to ECCT can generally be predicted based on cell type, degree of malignancy, and positive receptors for estrogen and progesterone hormones, as well as HER2. Hormone and HER2 negative receptors (triple negative) with a high degree of malignancy (grade 3) are generally the type with the best response to ECCT.
Cell types with strong estrogen (ER), progesterone (PR), and HER2 positive hormone characteristics generally have the lowest response to ECCT therapy. For these types, in addition to using the device, target medications are needed to block the receptors that trigger cancer cell growth. Hormone and HER2 receptors are ligand-activated, unlike ion channels which can be blocked or activated directly by electrical voltage. For hormone and HER2 positive types, ECCT can still provide a good response if the expression level is relatively not strong and the lump size is still relatively small (less than 1–2 cm), depending on the position. For relatively large sizes, dead cell removal generally cannot proceed well and completely, so if the trigger factors are high (strong ER, PR, HER2 positive), recurrence will be easy.
For cases without complete biopsy and IHC data, such as Mrs. Margareta’s case, observing excretion reactions serves as a quick and easy indicator. If excretion does not occur well after 2-3 weeks, it can be concluded that the cancer type is not one that responds well to ECCT; it would be more prudent to immediately decide to combine with medical therapy (surgery accompanied by chemotherapy/radiation). Generally, combining with surgery, if possible after 2-3 months of use for cases with minimal excretion levels, will accelerate the achievement of remission.
For over 10 years since her initial cancer diagnosis, Mrs. Margareta has hardly ever appeared seriously ill; her general condition is relatively normal, and her daily activities are normal at her pharmacy in Kaleno Warno City, Southwest Sumba. She never seemed ill. She had stopped using the device because scan results showed no abnormalities. Only during the pandemic, some time after vaccination, did she begin to feel a recurrence in the keloid area around the site of the previous needle biopsy. Ultrasound results showed the lump reappeared. Therefore, she began regularly using the ECCT device again. It took approximately one year until the mass disappeared again and was declared clear again, with only the keloid remaining. The doctor who examined her in Penang said no action was needed and advised her to continue using ECCT for prevention to avoid recurrence.
After 13 years since her initial breast cancer diagnosis, or 11 years since first using ECCT, Mrs. Margareta is in good health and normal condition, carrying out daily activities and traveling both domestically and abroad without issues. We hope Mrs. Margareta (WS) remains healthy.